Hospitals continue to close because they are not financially viable under the current system. Medical research has vastly improved our ability to prevent and treat serious illness; however, the payment for improved services has not kept pace with the interventions. While our doctors and hospitals can provide the gold standard of care, they receive copper for compensation.
The response has been both reflexive and whimsical. Hire consultants with no knowledge of health care, pass legislation increasing closure notification to Pennsylvania Department of Health from 90–180 days. Establish yet another agency to bring greater “accountability to both for profit and nonprofit health care profiteers.”
To be sure, venture capitalists can be involved in the demise of hospitals. One can buy a failing hospital and manage it in a way that optimizes their short time financial reporting. One can defer maintenance, cut service lines, short inventory, shrink employee benefits. Cutting operating expenses will enhance the income statement and the failing hospital has been turned around. It can then be bundled with other turned-around hospitals, and sold for a profit.
READ MORE — Parenting resources and support celebrated by clients of Pregnancy Resource Centers
In 2017, Community Health Systems (CHS), which is traded on the New York Stock Exchange, sold five hospitals in southeastern Pennsylvania to Tower Health for $418 million. Before their acquisition by CHS, Brandywine and Jennersville had been independent.
Why have long-standing, essential community assets become prey for predatory acquisition? Because operating as an ongoing hospital costs more than the income they generate from operating as a hospital.
Beyond the turning of the provision of health care into a commodity to be bundled, brokered and speculated, there are other drivers of the contraction of health care in the US. The compensation for providing care has not kept pace with the cost of the care.
Almost all the Philadelphia area health systems have negative operating margins, as reported by Harold Brubaker of the Philadelphia Inquirer. Only the Penn Health System and the Children’s Hospital of Philadelphia have positive operating margins of two percent and eight percent respectively.
Hospitals are closing because they lose money operating. Yet, paradoxically, we are spending more every year on health care. In the period 2009–2019, national per capita expenditure in constant dollars percentage increase ranged from 3.4 percent in 2015 to 4.3 percent in 2009, according to the CDC. We have become comfortable with and accepted the idea that we are spending too much on health care and we need to limit the increase.
In 1980, the increase in per capita spending was twelve percent. So how can we spend even more per capita, yet hospitals are closing for lack of funds? Is this simply bad management?
The magical thinking that we can drive a Lamborghini at Kia prices leads to increasing bureaucracy, price fixing, and regulatory burden.
One reason is payer mix. The insurance mix of Medicare, Medicaid, private insurance and self-pay of the patients treated by the hospital is a complicated system. Federal and state programs, Medicare and Medicaid set and decide how much to pay for the health care provided. This is a political decision, and the consensus is we are paying too much for health care.
Medicare only pays 84 cents for every dollar of care provided and Medicaid reimburses only 88 cents for every dollar spent, according to the American Hospital Association. Hospitals make up the shortfall of government payment for services by private insurance billing. For a hospital to survive, every Medicare patient seen and treated for a loss of sixteen cents must be balanced by a private patient providing a sixteen-cent profit. The payer mix of the catchment area of the hospital is critical to survival. Areas with higher Medicaid, Medicare and self-pay populations are challenged to stay open.
A more significant reason for the operating loss is the change in services provided, commonly referred to as the “market basket of goods” by economists.
In order to make a diagnosis, patients will frequently get an image such as an x-ray. In the 1970s, to image a patient’s brain, we inserted a needle into the carotid arteries, injected contrast dye, and took a rapid series of x-rays. The procedure was painful, noisy, dripped with complications, and provided sparse information. (Think of the scene in The Exorcist where Meagan has the study.) We now can image the brain and entire body using CT and MRI scans harvesting a tsunami of information all with an order of magnitude and less risk and complications. The cost of the now ubiquitous CTs and MRIs dwarf the expenditures for the needles, dye, and x-rays.
In the 1980s, a heart attack was treated with morphine, oxygen, and drugs for irregular heart-beats. It was not very effective, but it was not very expensive. Today, the standard of care for the acute heart attack is percutaneous angioplasty within 90 minutes. Consider the cost to build, equip, maintain, and staff with on-call, high professional personnel the catheterization lab. The ongoing expense to provide this care seismically dwarfs our 1980s best-of-care. The results are equally dramatic.
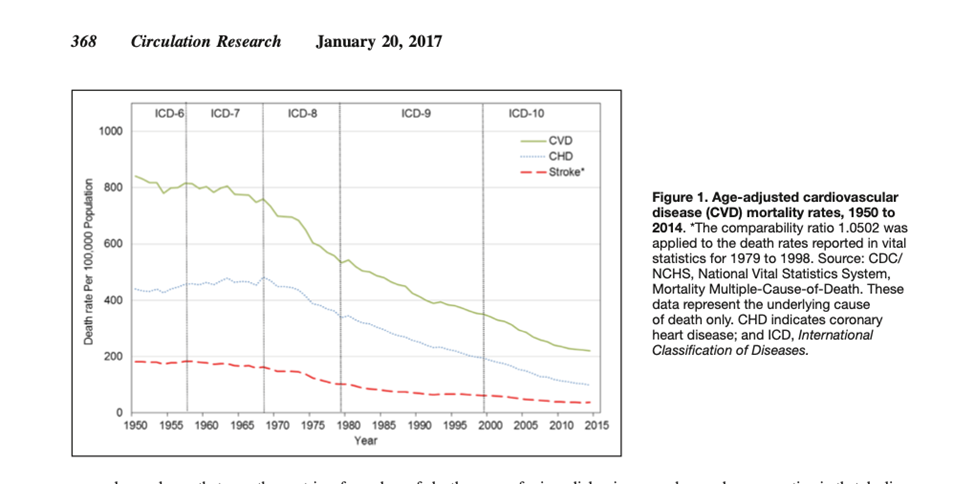
In Jan. 2017, Circulation Research published an article documenting the continuing decline in cardiovascular mortality in the US seen below.
Analogously, we buy a car for transportation as we purchase health care for our well-being. With cars, we may purchase a Kia or we may purchase a Lamborghini. I think it is unreasonable for us to assume we can drive a Lamborghini at Kia prices. In buying a Lambo over a Kia, we are choosing a different “market basket of goods.” Compared to the health care we had in the 1970s, we are roaring along in a Lambo.
We may choose to flatten the rising expenditures for the improving market basket of health care goods by setting Medicare and Medicaid reimbursements below the cost of services. If we choose to do so, as we have, we may expect shortages, wait lines, arbitrage and black markets. The shortages may range from cancer drugs to hospitals. The magical thinking that we can drive a Lamborghini at Kia prices leads to increasing bureaucracy, price fixing, and regulatory burden.
This approach, while having the virtue of being simple, easy, and signaling care, solves no problems. It only accelerates the mismatch expense and compensation for care provided. Solving the problem starts with understanding the problem — understanding based in economics, not whimsy.
Dr. Frank Speidel is a former emergency physician, US Navy Flight Surgeon and recovering hospital administrator (CEO). He is currently a producer and host of “The Doctor Is In” for MLTV 21.
Independence Blue Cross is a huge problem.
Doctors around the country complain about Medicare being the worst payer, but in Philadelphia Medicare is the best payer – solely because IBX pays so little.
IBX is turning eastern Delco into a medical desert.
Medicare has increased its rates
IBX and out of area actually pay reasonably well and better than medicare for procedures.
Aetna pays pays 50% of medicare rates for outpatinet
UNited health care and cigna about 70%
IBX is an adjunct of the Philadelphia Democrat Party.
Philly public school teachers are so well insured they can solicit medical opinions like medical tourists. Philly governance uses its leverage on IBX to give the unions sweetheart deals in lieu of cash.
Then IBX shifts the costs of this racket to the landscapers and hairdressers of Delco. That’s why they pay so much for so little coverage.
Ask the doctors of DCMH and Crozer about IBX reimbursement.
There ought to be tar and featherings.